


Pandemic Theater, The Anniversary Edition
When does "absence of evidence" start implying "evidence of absence"?

We’ve all seen examples of pandemic theater: precautions that seem misguided or overly-cautious given what we know about transmission mechanisms. Yesterday, I learned about a case that might be among the weirdest ones I’ve ever encountered, and arguably one of the funniest. Of all places, it happened in my son’s (recently reopened) school, in an area that’s full of great teachers, dedicated staff, highly-educated parents, and an involved school board. Luckily, it was not consequential. But still, it shows that we really haven’t found our bearings.
My son’s example came on the heels of something else I learned yesterday. Apparently, some libraries in the United States are still “quarantining” books for as long as 14 days before checking in and recirculating them.


These examples of lengthy library quarantines came in response to a Twitter thread of mine, highlighting a fascinating study that had caught my attention about a mystery transmission case in New Zealand that I had been tracking.


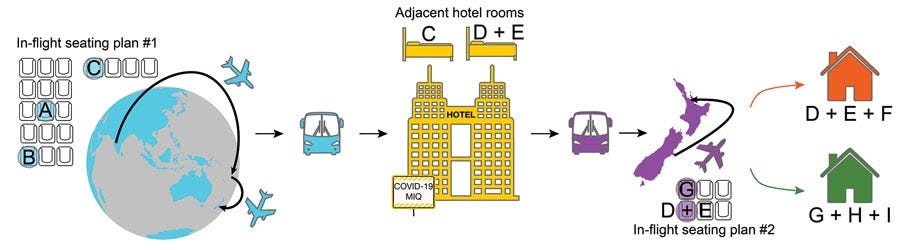
In this newly-published study, scientists in New Zealand examined in detail one of the few suspected cases of fomite transmission—transmission through touching a surface. A traveler quarantined in a hotel had infected someone else also quarantined in the same hotel, and, for the longest time, suspicions had fallen on a lid on a garbage bin. The hotel has close-circuit TV though so they could trace when people had touched what, and it turns out that the most likely scenario is that the infection occurred via aerosol transmission that happened when doors to both the hotel rooms—facing the same corridor—were briefly open at the same time when the travelers were being swabbed without masks.
Nevertheless, footage showed that during routine testing on day 12, which took place within the doorway of the hotel rooms, there was a 50-second window between closing the door to the room of case-patient C and opening the door to the room of case-patients D and E. Therefore, we hypothesized that suspended aerosol particles were the probable mode of transmission in this instance, and that the enclosed and unventilated space in the hotel corridor probably facilitated this event (4). A commissioned review of the ventilation system found that the rooms in question had a net positive pressure compared with the corridor. Fomite transmission through use of communal bins in the corridor was considered to be a less probable route of transmission because contact with the bin lid by case-patient D was >20 hours after it was touched by case-patient C.
New Zealand, of course, has been comparatively very successful in containing the coronavirus. It’s pretty amazing how a country can do precise tracking when there is so little transmission otherwise. In the United States, we’d have ended up throwing up our hands, probably, because the more the community transmission, the harder it is to devote this much energy to a case. (They also did genomic sequencing so we are sure that these people were infected in the same chain).
The study was notable not just because it knocked down one of the few known and strongly-suspected cases of fomite transmission, but because it showed, once again, that aerosol transmission can occur even during very brief periods and over long distances. For clarity: most aerosol transmission also occurs near the person doing the exhaling/talking/singing—producing those aerosols. However, these “floaty” particles can also linger, waft, get around, especially in poorly ventilated spaces, and accumulate. Also, the longer people share air in an enclosed space, the more likely the transmission.
A case like this doesn’t mean that every 50- second encounter is certain to create transmission, but it shows that it’s possible, emphasizing something that’s been perplexingly uphill to communicate: we need to pay more attention to ventilation and aerosols, and less to “deep cleaning” and fomites. Here’s an interview I did months ago, and I could probably repeat it all today and receive the same influx of frustrated emails from victims of pandemic theater: people in workplaces with excessive cleaning and plexiglass, but where workers are not allowed to open windows and where people take off their masks if they are separated by six feet.


But all this brings an interesting meta-epistemological point, too. Were we always wrong to take these extra fomite precautions? When should we have adjusted? When is the precautionary principle reasonable, when is it excessive? How should we think about all this?
There is a phrase I’ve used a lot in the last year: “absence of evidence isn’t evidence of absence.” It’s generally true and it’s an important corrective to a tendency we sometimes see in medicine and in science where a scientist or a press person states “there is no evidence that X causes Y,” when what they actually mean is that is that we don’t yet know if X causes Y. Maybe it does, maybe it does not. The phrasing is important because the way language works colloquially—how it operates in the world—means that “there is no evidence that X causes Y” uttered by scientists is heard by many people as “X does not cause Y.” (We also saw this play out when the suggestion that “no evidence that vaccines block transmission” got misinterpreted widely as “vaccines do not block transmission.”)

But of course, if you keep looking hard for something for a whole year, and end up not finding much, if any, at some point absence of evidence does start implying evidence of absence. Like many other “rules” of causal inference and decision-making under uncertain conditions, “absence of evidence is not evidence of absence” is not a simple, absolute rule that can be applied without context or consideration. (Another non-favorite: the often-dropped maxim that “correlation does not imply causation.” Well, it can indeed imply just that. In fact, it often does, except when it doesn’t! Also, sometimes the plural of anecdote is, indeed, data. But I digress. Those are all subjects for future posts.)
I also took all the extra precautions last year too early on, in February or early March 2020, when things were unclear. I did not let relative dearth of evidence on transmission mechanisms stop me from undertaking what were—in hindsight—excessive precautions, especially since that absence was paired with lack of knowledge on the downsides of being infected. Even though I wasn’t overly concerned for myself, I also wanted to be sure I wasn’t a link in a potential transmission chain! In February 2020, we still had a poorly-understood disease from a novel pathogen with then-unclear patterns of transmission. It made sense to be extra careful and throwing the kitchen-sink, so to speak, at everything we could target.
So I let the boxes delivered to my home sit in the sun before taking them in. I hand-sanitized often and basically avoided as much contact as I could, even outdoors. Then, as the epidemiology and other data came in—and it came in very fast—I both relaxed and tightened up. I ceased quarantining boxes and started socializing outdoors. At the same time, I was more careful in other dimensions. I refused to go into a grocery store if it looked overly-crowded or if it wasn’t enforcing mask requirements. I started masking up even more strictly if I was indoors, but more casually—more as a courtesy—if outdoors. By the end of March 2020, I felt confident enough to write my first article pleading with authorities to keep parks open.
In the short run, closing parks may seem prudent, when our hospitals are overrun and we are trying so hard to curb the spread of COVID-19. But in the medium to long run, it will turn out to be a mistake that backfires at every level. While it’s imperative that people comply with social-distancing and other guidelines to fight this pandemic, shutting down all parks and trails is unsustainable, counterproductive, and even harmful.
By the end of April 2020, I was comfortable enough to let “absence of evidence” function as “evidence of absence” for practical purposes for dealing with surface transmission:
Well, yesterday, a year after my son’s school closed to all in-person instruction, it opened again. This week it will be hybrid—students are in-person in cohorts—and then it will close for a week. And then it will open up for four days per week in early April (and it will no longer be hybrid, though Wednesdays will remain virtual). My area has very low community transmission. Vaccination opened to teachers a month ago. Every classroom has windows and doors that can open, often a patio attached to the classroom. There is a large schoolyard and the weather is pleasant and mild. Children are also allowed to continue fully remote if a family wishes. All good.
When my son got back from school yesterday, I eagerly listened to how his day went. The very first class on their very first day was physical education, he told me. And then an astonishing tale of pandemic theater had unfolded. The students were instructed to sit in front of their individual computers. Through their screens, a physical education teacher played videos which instructed them to “jump around,” “kick right foot,” “now kick the left foot,” and such. They were supposed to “exercise” together. Inside the classroom. They were all wearing masks, but we know that exercise increases aerosol production. And the kind of masks children wear are not likely to be correctly-worn N95s.
While I had no qualms sending my son back to school, especially given the conditions in my area, I didn’t expect their very first class back after a year to be filled with huffing and puffing in an indoor space.
Luckily, their fifth-grade energy thwarted our attempts to further bungle the way we have misordered our COVID mitigations.
My son calmly explained that, faced with instructions to exercise indoors, every single student had promptly turned off their screens—remember, they’re doing blended education, so that the students in the school are just sitting in front of the screen along with students at home. The screen teacher could no longer see the students. The kids then sat still for the duration of the PE class, not getting up out of their seats, let alone exercising. He would not comment on the amount of snickering and eye-rolling that may or may not have occurred. What about the supervising teacher, I asked? (They have someone who sits in the classroom even when someone else is “instructing them” through the screen). That person, too, had reciprocated their wisdom by also ignoring the person on streaming video urging them to jump, kick and turn around, and also ignoring the obvious reality: none of the students were.
I would have let that go except for noticing that he had registered a good amount of exercise for the day through our shared watch app—he is not into “competing” with me through the app, but we enjoy comparing our exercise levels. If he had wisely sat out indoor PE, what was all that? Oh, that, he shrugged. Students were, sensibly, let loose outside for lunch, he explained, and they spent the whole hour playing “infection”—essentially a game of tag, but with a pandemic theme.
Better that, I guess, than the pandemic theater games we seem reluctant to let go of.
On that note: what’s your pandemic theater example?
My favorite (read: most frustrating) pandemic theater example is on my TV screen every evening since the NCAA tournament started.
College basketball coaches are (seemingly) told to wear masks while they're on the sidelines coaching their teams. From what I've seen, all have dutifully complied. However! As soon as the game starts and they need to do their jobs, these coaches routinely, and almost without fail, will pull down their (mostly cloth) masks to shout loudly at their players and at the referees. It makes wearing the masks the rest of the time nearly irrelevant! Why even have them wear masks if they're going to pull them down and aerosolize every few minutes anyways? It's not protecting them OR the people around them!
That ending is the funniest thing I've read in a while (and I've spent this whole year watching my daughter and her cousins and their occasional friend visits develop their own versions of "pandemic" involving distancing) but also I somehow had no idea you had a kid and am now not-very-usefully ruminating on the question "How does Zeynep get so much done?!"
I homeschooled my kids, so we didn't witness any of the theater in the classrooms, though I'm sure there was plenty. A doctor friend of ours did call my spouse somewhere during lockdown last spring to ask how long he though he should microwave his newspaper for. Though as in your first examples, fair enough back when when we didn't know very much.
My mother-in-law was in a rehabilitation facility in the UK for a few months this winter, where there was plenty of hygiene theater from the care staff, but a dementia resident in the home wandered around at will all the time, and came into my mother-in-law's room almost every day and sat on her bed thinking she was a relative. Which is how my mother-in-law got Covid. Luckily she'd had the AZ vaccine a few days before she got the virus, so it (we think) mitigated the effects, though she was still very sick.